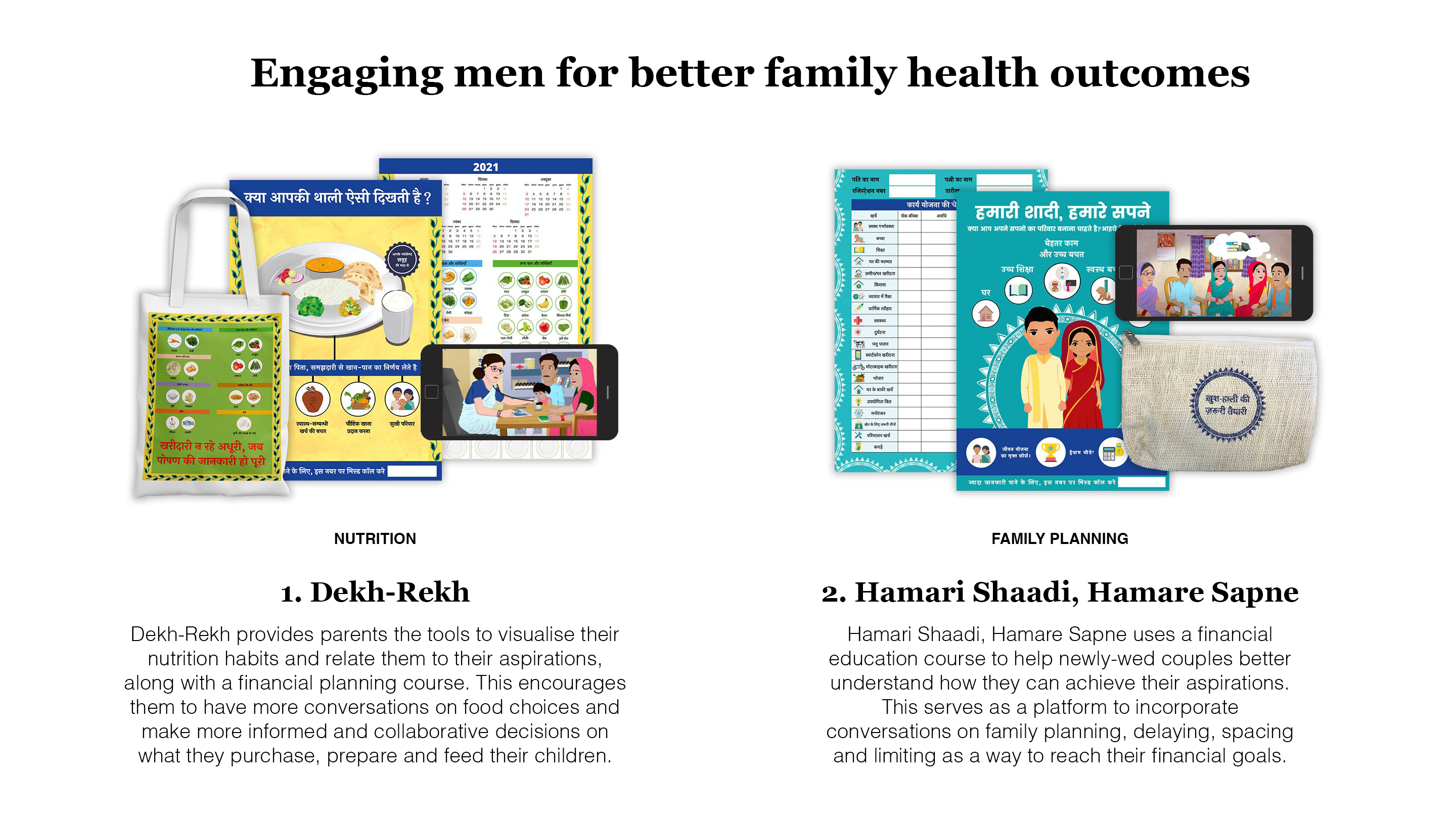
Engaging men for better family health outcomes




Team
Company | Institution
Category
Type
Project description
Engaging men in family planning and nutrition programming provides an opportunity to move towards better health and gender outcomes. To meet this goal, we designed two innovative programs in rural Bihar, India, using Human-centered Design (HCD) research, co-creation, and prototype testing, grounded in behavioral science approaches.
The first, Dekh-Rekh (“Care and Nurture”) provides couples with tools to visualize their nutrition habits and relate them to their aspirations, encouraging more informed and collaborative decisions on what couples purchase, prepare and feed their children.
The second, Hamari Shaadi, Hamare Sapne (“Our Marriage, Our Dreams”) uses a financial education course for newly-wed couples to introduce conversations on contraceptives, delaying, spacing and limiting as a way for couples to reach their financial aspirations.
In both programs, trained couples from the community deliver the programs to enrolled couples, acting as role models for participants, while creating an open environment to talk about sensitive issues.
A learning pilot with 2000 households demonstrated the immense potential these programs have to change health and gender outcomes, and we hope to scale these two programs to achieve lasting behavioral change. Through a public launch event in the capital city of Delhi, we have shared learnings with key stakeholders and policymakers, and, already, India’s National Ministry of Health and Family Welfare in India has made engaging men in family planning a top priority for their 2030 vision, citing our report as a key resource in support of this mission.
Learn more: https://www.engagemen.in/
Project Description
Family planning and child nutrition indicators show the least improvement of health indicators across India. Historically, programs in these two sectors have focused on women, both as end-users and as providers (e.g. female community health workers). While many of these programs have seen considerable success in their outcomes, challenges have emerged in the long run:
- They place a disproportionate burden on women, both as end-users and as the ones delivering health programs.
- They reinforce the imbalanced gender norms that underlie women’s unpaid care work and time poverty and, relatedly, their mobility and workforce participation.
- Men have been further alienated from the “female” domains of family planning and nutrition.
Evidence shows positive improvements in health, nutrition, and gender outcomes when men’s engagement increases, but falls short of showing lasting behavior change at scale. To fill this gap, teams from Dalberg and Project Concern International India set out to design programs, answering the question: How might we engage men in nutrition and family planning through innovative and gender transformative programs in rural Bihar?
We developed and tested two programs over 2.5 years. We used an interdisciplinary approach anchored on human-centered design research and behavioral science, supported by literature reviews, expert interviews, rapid prototype testing and a learning pilot to design and test innovative programmatic solutions. Soon after we began ideating on potential programs, the pandemic began, prompting us to adopt a hybrid between remote and in-person research and work closely with community representatives as partners in prototyping and piloting the programs. This provided nuanced insights and shaped the programs greatly.
From 30+ program ideas, we narrowed to 2 final programs whose target audience was young, zero- or one-parity couples in rural Bihar (a state in North India). Our nutrition-focused program, called Dekh-Rekh (“Care and Nurture”), leads couples towards making more healthy, informed food choices and purchases for their children. The family planning-focused program, Hamari Shaadi, Hamare Sapne (“Our Marriage, Our Dreams”), creates a comfortable environment for couples to discuss the often taboo topics of contraception, delaying, spacing and limiting by using a financial planning course as an entry-point.
Findings from our learning pilot with 2000 households show the immense potential of these programs to change couples’ family planning and nutrition behaviors. For instance, our intervention villages saw a net 30% point increase in children’s minimum dietary diversity; and 16% point increase in modern contraceptive use. We also saw shifts in gender-related behaviors and spousal communication, including a net increase of 18% points in men’s involvement in feeding their children, a behavior typically divided by gendered, and a 16% point increase in women reporting greater support from their husbands on contraceptive use.
Lastly, our cross-disciplinary and iterative approach to designing, developing, and implementing programs could serve as a model for other sectors, while our strong gender lens provides lessons for gender-sensitive programming. Our partnerships with community members and local institutions during research and implementation offer lessons on the potential of community participatory research, and building system capacity and inter-community trust.
The first, Dekh-Rekh (“Care and Nurture”) provides couples with tools to visualize their nutrition habits and relate them to their aspirations, encouraging more informed and collaborative decisions on what couples purchase, prepare and feed their children.
The second, Hamari Shaadi, Hamare Sapne (“Our Marriage, Our Dreams”) uses a financial education course for newly-wed couples to introduce conversations on contraceptives, delaying, spacing and limiting as a way for couples to reach their financial aspirations.
In both programs, trained couples from the community deliver the programs to enrolled couples, acting as role models for participants, while creating an open environment to talk about sensitive issues.
A learning pilot with 2000 households demonstrated the immense potential these programs have to change health and gender outcomes, and we hope to scale these two programs to achieve lasting behavioral change. Through a public launch event in the capital city of Delhi, we have shared learnings with key stakeholders and policymakers, and, already, India’s National Ministry of Health and Family Welfare in India has made engaging men in family planning a top priority for their 2030 vision, citing our report as a key resource in support of this mission.
Learn more: https://www.engagemen.in/
Project Description
Family planning and child nutrition indicators show the least improvement of health indicators across India. Historically, programs in these two sectors have focused on women, both as end-users and as providers (e.g. female community health workers). While many of these programs have seen considerable success in their outcomes, challenges have emerged in the long run:
- They place a disproportionate burden on women, both as end-users and as the ones delivering health programs.
- They reinforce the imbalanced gender norms that underlie women’s unpaid care work and time poverty and, relatedly, their mobility and workforce participation.
- Men have been further alienated from the “female” domains of family planning and nutrition.
Evidence shows positive improvements in health, nutrition, and gender outcomes when men’s engagement increases, but falls short of showing lasting behavior change at scale. To fill this gap, teams from Dalberg and Project Concern International India set out to design programs, answering the question: How might we engage men in nutrition and family planning through innovative and gender transformative programs in rural Bihar?
We developed and tested two programs over 2.5 years. We used an interdisciplinary approach anchored on human-centered design research and behavioral science, supported by literature reviews, expert interviews, rapid prototype testing and a learning pilot to design and test innovative programmatic solutions. Soon after we began ideating on potential programs, the pandemic began, prompting us to adopt a hybrid between remote and in-person research and work closely with community representatives as partners in prototyping and piloting the programs. This provided nuanced insights and shaped the programs greatly.
From 30+ program ideas, we narrowed to 2 final programs whose target audience was young, zero- or one-parity couples in rural Bihar (a state in North India). Our nutrition-focused program, called Dekh-Rekh (“Care and Nurture”), leads couples towards making more healthy, informed food choices and purchases for their children. The family planning-focused program, Hamari Shaadi, Hamare Sapne (“Our Marriage, Our Dreams”), creates a comfortable environment for couples to discuss the often taboo topics of contraception, delaying, spacing and limiting by using a financial planning course as an entry-point.
Findings from our learning pilot with 2000 households show the immense potential of these programs to change couples’ family planning and nutrition behaviors. For instance, our intervention villages saw a net 30% point increase in children’s minimum dietary diversity; and 16% point increase in modern contraceptive use. We also saw shifts in gender-related behaviors and spousal communication, including a net increase of 18% points in men’s involvement in feeding their children, a behavior typically divided by gendered, and a 16% point increase in women reporting greater support from their husbands on contraceptive use.
Lastly, our cross-disciplinary and iterative approach to designing, developing, and implementing programs could serve as a model for other sectors, while our strong gender lens provides lessons for gender-sensitive programming. Our partnerships with community members and local institutions during research and implementation offer lessons on the potential of community participatory research, and building system capacity and inter-community trust.